Don't miss Hallway Huddle - Chronic kidney disease in type 2 diabetes
I don't understand why it can cause hyperkalemia. Even more... from my point of view... it could cause hypokalemia... Do you have an explanation.
Sylvie Bertrand MD, CSPQ, FRCP(c)
Endocrinologist
Montreal
Sylvie Bertrand MD, CSPQ, FRCP(c)
Endocrinologist
Montreal

11 years ago
·
#551 Hello,
Firstly, sorry for the delay in this reply.
I agree with you; the mechanism of hyperkalemia is not well understood and counterintuitive. The impact on patients with preserved renal function is only very mild. Important hyperkalemia appears to be limited to those with more advanced renal failure, a group that would not commonly be treated with an SGLT2 inhibitor for diabetes care, based on the current label.
Here is a summary of the findings with Invokana:
It is not clear whether this effect (which was seen more-so in patients with impaired renal function) was independent in small changes in GFR or volume status. One possibility therefore, is that a slight reduction in volume status led to a reduction in sodium delivery to the cortical collecting duct in the distal nephron, resulting in less sodium exchanged for potassium. However, this would be speculation.
I have reviewed this finding with one of our local potassium experts (he's an internationally recognized authority), and he was similarly surprised by the finding of hyperkalemia.
Perhaps the lesson here is to repeat electrolytes and renal function shortly after starting the medication, a practice that is likely common irrespective of this finding. One could consider a low potassium diet for those with more borderline renal function. You can download an example diet here:
Low Potassium Diet
Firstly, sorry for the delay in this reply.
I agree with you; the mechanism of hyperkalemia is not well understood and counterintuitive. The impact on patients with preserved renal function is only very mild. Important hyperkalemia appears to be limited to those with more advanced renal failure, a group that would not commonly be treated with an SGLT2 inhibitor for diabetes care, based on the current label.
Here is a summary of the findings with Invokana:
- Mean percent changes from baseline in blood potassium were 0.5% and 1.0% for INVOKANA™ 100 mg and 300 mg, respectively, compared to 0.6% for placebo. Episodes of elevated serum potassium (> 5.4 mEq/L and 15% above baseline) were seen in 4.4% of patients treated with INVOKANA™ 100 mg, 7.0% of patients treated with INVOKANA™ 300 mg, and 4.8% of patients treated with placebo.
- In a trial in patients with moderate renal impairment (eGFR 30 to < 50 mL/min/1.73 m2), increases in serum potassium to > 5.4 mEq/L and 15% above baseline were seen in 16.1%, 12.4%, and 27.0% of patients treated with placebo, INVOKANA™ 100 mg, and INVOKANA™ 300 mg, respectively. Elevations to ≥ 6.5 mEq/L occurred in 1.1%, 2.2%, and 2.2% of patients treated with placebo, INVOKANA™ 100 mg, and INVOKANA™ 300 mg, respectively.
It is not clear whether this effect (which was seen more-so in patients with impaired renal function) was independent in small changes in GFR or volume status. One possibility therefore, is that a slight reduction in volume status led to a reduction in sodium delivery to the cortical collecting duct in the distal nephron, resulting in less sodium exchanged for potassium. However, this would be speculation.
I have reviewed this finding with one of our local potassium experts (he's an internationally recognized authority), and he was similarly surprised by the finding of hyperkalemia.
Perhaps the lesson here is to repeat electrolytes and renal function shortly after starting the medication, a practice that is likely common irrespective of this finding. One could consider a low potassium diet for those with more borderline renal function. You can download an example diet here:
Low Potassium Diet
It is also known two other adverse effects namely, orthostatic hypotension and dehydration. Thus, it's very reasonable to understand why there is hyperkalemia and not hypokalemia as I first thought.
Seems like the glucose and sodium exerts it's osmotic effect and results in dehydration, which would cause hyper kalemia.
Seems like the glucose and sodium exerts it's osmotic effect and results in dehydration, which would cause hyper kalemia.
7 years ago
·
#1378 But wouldnt the dehydration cause a low volume state and with it a decrease in renal plasma flow and activation of the RAAS sodium rabsorption and potasium secretion.
7 years ago
·
#1379 But wouldnt the dehydration cause a low volume state and with it a decrease in renal plasma flow and activation of the RAAS sodium rabsorption and potasium secretion.
If a patient is pre-renal and distal sodium delivery is low as a result (to conserve volume), then even if aldosterone acts, there is little sodium to participate in potassium exchange. If this physiology didn't occur, we would be come hypokalemic whenever volume contracted.
Dr. Jordan Weinstein
The hyperkalemia is caused by the lack of stimulation of the Na+/K+ ATPase on the basolateral side of the PCT cells. If SGLT2 is inhibited, then there is less glucose and sodium being reabsorbed in the PCT. This means less Na+ available for the Na+/K+ pump on the basolateral side, leaving more K+ in the body.
7 years ago
·
#1624 The hyperkalemia is caused by the lack of stimulation of the Na+/K+ ATPase on the basolateral side of the PCT cells. If SGLT2 is inhibited, then there is less glucose and sodium being reabsorbed in the PCT. This means less Na+ available for the Na+/K+ pump on the basolateral side, leaving more K+ in the body.
I think this point is now moot. Hyperkalemia is not a feature of SGLT2 inhibitors across the large-scale clinical trials.
Dr. Jordan Weinstein
7 years ago
·
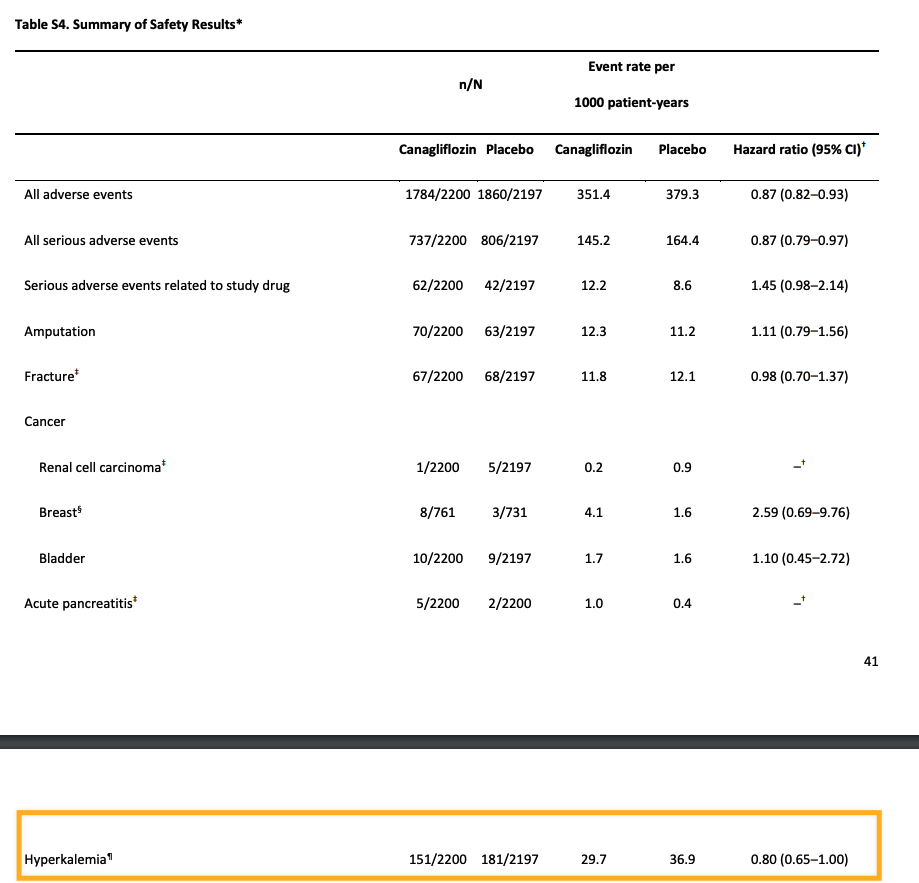
#1627 For those following this, in the latest CREDENCE study - where all patients were in ACE inhibitors or ARBS - there was actually a LOWER incidence of hyperkalemia in the SGLT2i group. Hyperkalemia is not a feature of these drugs.
See supplementary appendix:
https://www.nejm.org/doi/suppl/10.1056/NEJMoa1811744/suppl_file/nejmoa1811744_appendix.pdfhttp://d.brightbean.ca/q5aHMm+
Dr. Jordan Weinstein
See supplementary appendix:
https://www.nejm.org/doi/suppl/10.1056/NEJMoa1811744/suppl_file/nejmoa1811744_appendix.pdfhttp://d.brightbean.ca/q5aHMm+
Dr. Jordan Weinstein
7 years ago
·
#1628 For those following this, in the latest CREDENCE study - where all patients were in ACE inhibitors or ARBS - there was actually a LOWER incidence of hyperkalemia in the SGLT2i group. Hyperkalemia is not a feature of these drugs.
See supplementary appendix:
https://www.nejm.org/doi/suppl/10.1056/NEJMoa1811744/suppl_file/nejmoa1811744_appendix.pdf
Dr. Jordan Weinstein
See supplementary appendix:
https://www.nejm.org/doi/suppl/10.1056/NEJMoa1811744/suppl_file/nejmoa1811744_appendix.pdf
Dr. Jordan Weinstein
5 years ago
·
#2445 This paper also addresses this issue. SGLT2i are pretty much potassium irrelevant 
https://link.springer.com/article/10.1007/s13300-015-0150-y
https://link.springer.com/article/10.1007/s13300-015-0150-y
- Page :
- 1
There are no replies made for this post yet.
LEADING RESOURCE IN NEPHROLOGY EDUCATION