These questions belong to Part 1 of our feature on Hot Topics in Hyperkalemia. Please find Part 2 at the following link
Q1. With CKD patients who had a first hyperkalemia (HK) episode, what is the approximate likelihood of a second HK event occurring?
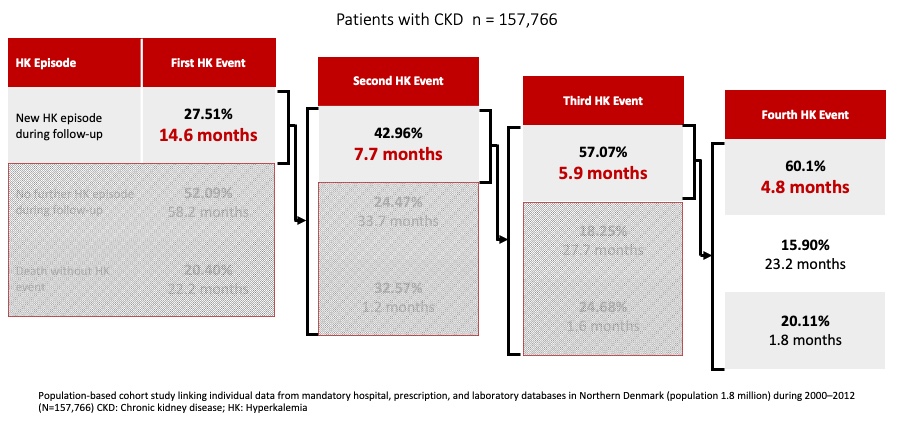
Patients with CKD and HF tend to have recurrent hyperkalemia episodes with successively shorter time between each subsequent episode. In a large population cohort study (n = 157,766) conducted in Denmark between 2000 and 2012, it was shown that among people with CKD that had a first HK event, 42.96% had a second event, with a median time between events of 7.7 months. Patient proportions who experienced a third (57.07%) or fourth (60.10%) hyperkalemia event after previous events were even greater. Similar observations were made among HF patients1[Thomsen 2018, p. 1614/fig.2].
Reference:
- Thomsen RW, Nicolaisen SK, Hasvold P, et al. Elevated potassium levels in patients with chronic kidney disease: occurrence, risk factors and clinical outcomes-a Danish population-based cohort study. Nephrol Dial Transplant. 2018 Sep 1;33(9):1610-1620. doi: 10.1093/ndt/gfx312.
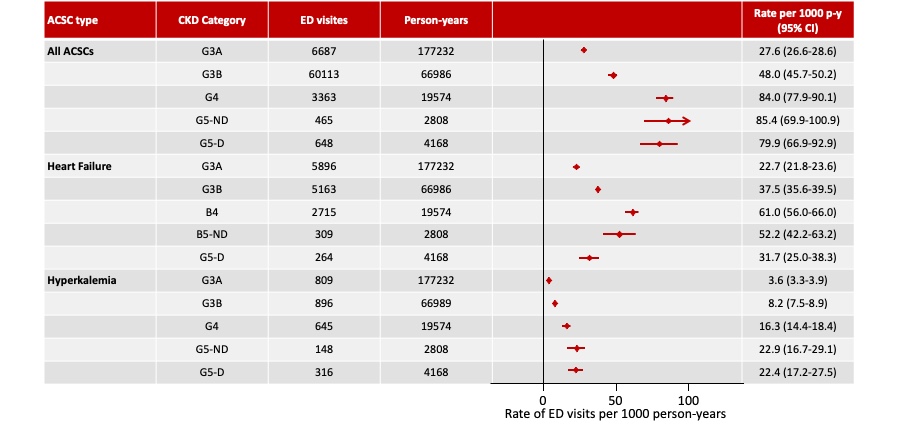
Q2. What is the impact of hyperkalemia on the number of ER visits among CKD patients in Canada?
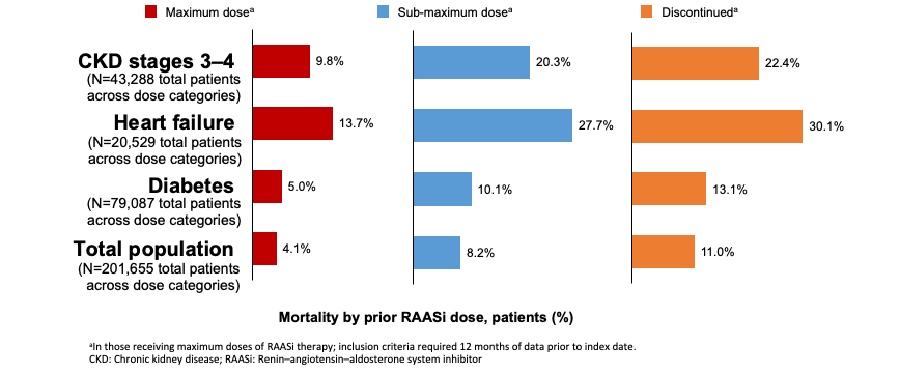
Q3. Knowing that suboptimal dosing of RAASi should be avoided, how does hyperkalemia impact one’s ability to reach targeted RAASi treatment for patients?

Q4. The clinical data supporting the use of SPS is limited. Should we be revisiting the use of SPS for hyperkalemia management?
Q5. How frequent are GI side effects with SPS in real world setting and what does the recent data tell us about the risk associated with its use?

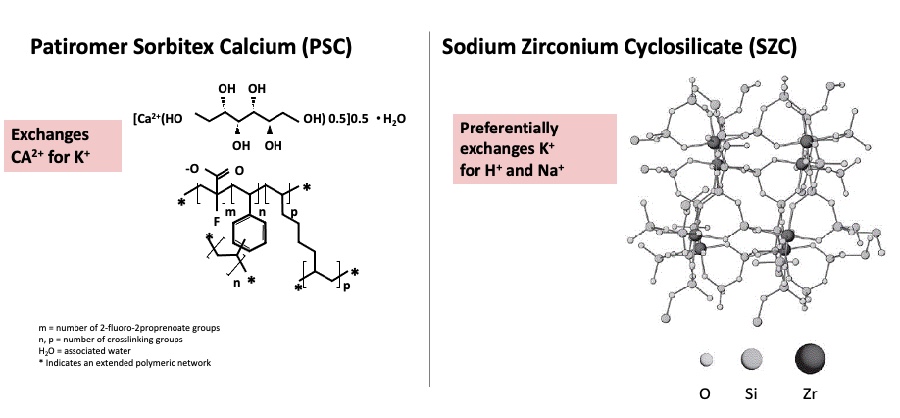
Q6. How do novel binding agents work?
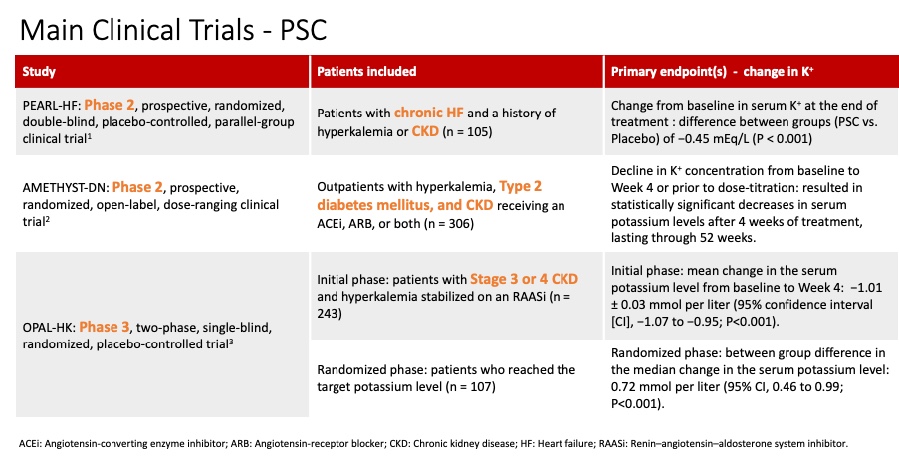
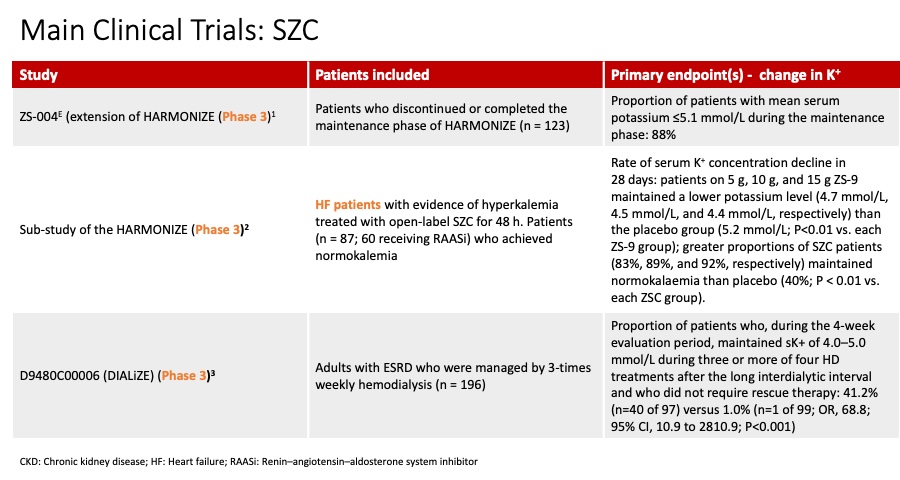
Q7. What does the clinical program look like for the novel potassium binders?


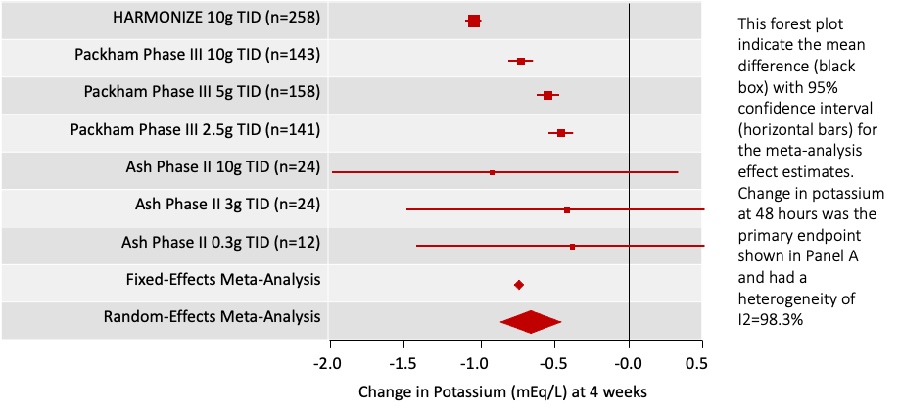
Q8. What type of data is available for correction of HK using novel potassium binders?

Q9. How well tolerated are novel potassium binders?
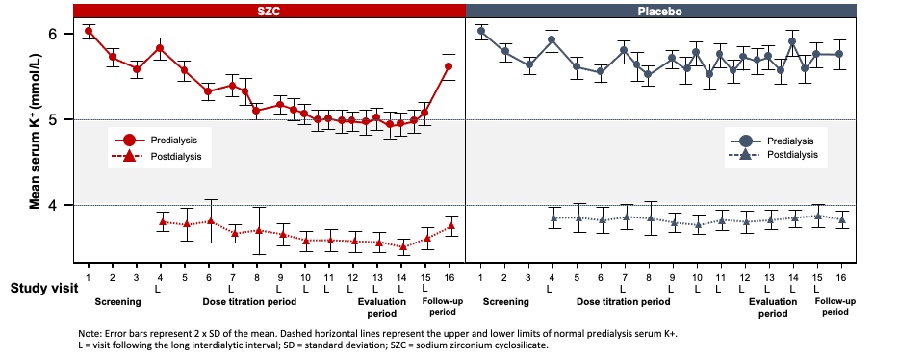
Q10. How can novel potassium binders help manage persistent predialysis hyperkalemia in chronic hemodialysis patients?