UKidney Nephrology News and Insights
Hypertension Update: Did you know...


Welcome to the Circle of Knowledge Program
Two Canadian experts, Dr. Jordan Weinstein and Dr. Louis Girard, nephrologists, will share how to translate clinical evidence into daily practice for optimal hypertension patient care.
Upon reflection, what percentage of the patients in your practice are on an optimal medication regimen in terms of dosing and medications selected?
Did you know that a recent study showed that 58% of the cases of resistant hypertension are due to a suboptimal medication regimen?
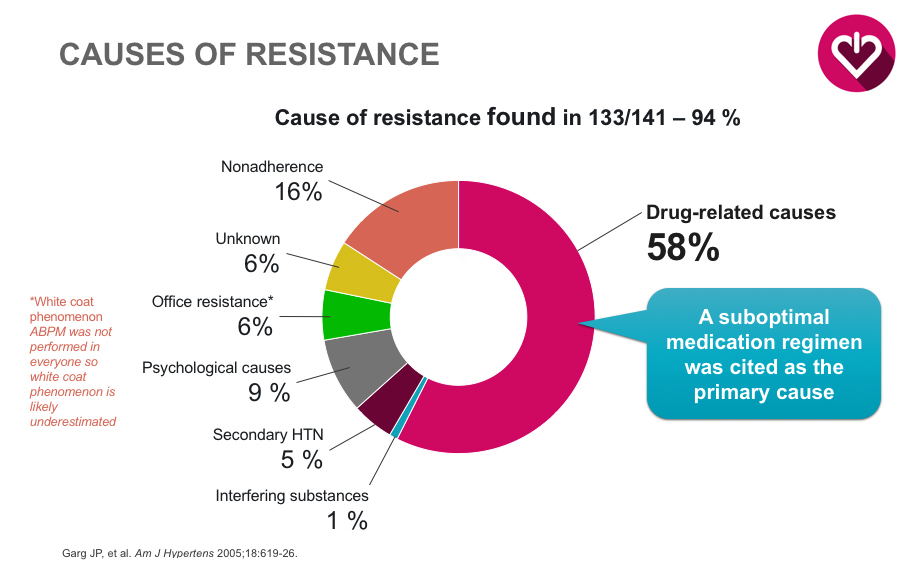 1281 patient with hypertension were studied. 141 met criteria for RH. The most common cause of RH was a suboptimal medication regimen (58%). Other notable causes included:non-adherence (16%), white coat hypertension (6%) and secondary hypertension (5%). Goal BP was most commonly achieved by optimization of diuretics and the addition of medications.
1281 patient with hypertension were studied. 141 met criteria for RH. The most common cause of RH was a suboptimal medication regimen (58%). Other notable causes included:non-adherence (16%), white coat hypertension (6%) and secondary hypertension (5%). Goal BP was most commonly achieved by optimization of diuretics and the addition of medications.
Did you know that a recent study found that 52% of patients with office SBP of 140 mmHg or below were actually uncontrolled in the morning before taking their meds?
What percentage of patients in your practice are at risk of CV events due to masked hypertension?
In this detailed review, the notion of “perfect blood pressure control” is introduced. The existing literature pertaining to CV and cerebrovascular eventsis highlighted. The take-home message suggests that despite at target BP measurements in the office or during the day at home, that patients may still be at increased risk for CV events. Specific situations where is has been studied include: nocturnal hypertension, absence of “nocturnal dipping” and early morning BP surges. Also, the more complex notion of BP variability and its association with CV events is reviewed. Therapeutic recommendations are proposed and will be reviewed below.
Did you know that the majority of CV events occur in the early morning hours?
Based on the above discussion, a particularly at risk period for patients appears to be the early morning hours. During this time, BP medications with a shorter half-life are wearing off. This also corresponds to the time at which the majority of CV events occur. The authors propose reducing this risk by using longer-acting diuretics. Additionally, longer acting medications such as ARBs and CCBs are useful agents in terms improving nocturnal/early morning BP as well as reducing BP variability.
When thinking about your patients, are there are opportunities to reduce CV events by increasing the utilization of long-acting anti-hypertensives?
Monthly Clinical Pearl
Hypertension remains a large problem for our patients. Despite the best efforts of care providers, many patients who are treated, continue to be at an elevated risk of CV events due to suboptimal medication regimens. Additionally, masked hypertension continues to be difficult to identify. There is a large body of evidence supporting the use of single once-daily pill combinations to achieve better blood pressure control via two mechanisms:
- The use of two medications will antagonize different pathways to achieve BP control
- Improved compliance.