UKidney Nephrology News and Insights

AUG
07
0
JUN
18

Welcome to the Circle of Knowledge Program
Two Canadian experts, Dr. Jordan Weinstein and Dr. Louis Girard, nephrologists, will share how to translate clinical evidence into daily practice for optimal hypertension patient care.
NOV
26
Previously, UKidney News reported a possible link between calcium channel blockers and the development of breast cancer. Data from the Intermountain Medical Center Heart Institute study were presented at the 2014 American Heart Association Scientific Sessions in Chicago, dispelling some of this concern:
"We found no robust data that calcium channel blocker medications increase a person's risk of breast cancer," said Jeffery L. Anderson, MD, a cardiologist and researcher at the Intermountain Medical Center Heart Institute. "Given the important role calcium channel blocker medications play in treating heart conditions, we think it's premature to discontinue their use. At this point we recommend that patients continue taking these medications to treat their hypertension."
While it is very difficult to ever prove a negative association, these data do provide some reassurance to a large number of patients using this important antihypertensive.
FEB
20
Welcome to the Circle of Knowledge Program
Two Canadian experts, Dr. Jordan Weinstein and Dr. Louis Girard, nephrologists, will share how to translate clinical evidence into daily practice for optimal hypertension patient care.
Upon reflection, what percentage of the patients in your practice are on an optimal medication regimen in terms of dosing and medications selected?
FEB
20
Welcome to the Circle of Knowledge Program
Two Canadian experts, Dr. Jordan Weinstein and Dr. Louis Girard, nephrologists, will share how to translate clinical evidence into daily practice for optimal hypertension patient care.
Hypertension is one of the most important risk factors for adverse health outcomes that we treat either in specialty or primary care. However, controversy has always existed in terms of the target blood pressure that clinicians should aim for when managing patients with different comorbidities. The SPRINT study published in 2015 continues to offer insight and some controversy guiding therapy in patients with hypertension particularly those at high cardiovascular risk.
The SPRINT Study was received with great fanfare when it was published on November 26th in the New England Journal of Medicine. The primary results, summarized in the publication’s abstract are these:
"Among patients at high risk for cardiovascular events but without diabetes, targeting a systolic blood pressure of less than 120 mm Hg, as compared with less than 140 mm Hg, resulted in lower rates of fatal and nonfatal major cardiovascular events and death from any cause, although significantly higher rates of some adverse events were observed in the intensive-treatment group."
The essential word in that abstract’s conclusion - and which prevents the application of these results - is ‘targeting’. The conclusion accepted by many is that aggressive blood pressure reduction, that is the achieved blood pressure, drove the observed results. However, it may well be that the act of targeting a low blood pressure, and using cardioprotective drugs to do so, explained the results rather than the reduction of blood pressure itself. And unravelling this nuance is the key to understanding whether SPRINT’s main message is applicable to the general population. I would argue that in its current form SPRINT suffers from a major methodological short-coming that leaves us in a quagmire.
Top-line results of the Symplicity 3 trial were revealed this week, showing that despite being safe, renal denervation was no better than a sham procedure at controlling blood pressure at 6 months. As reported on Medscape:
A report in JAMA - Internal Medicine[1] raises important safety concerns about calcium channel blockers, one of the most widely prescribed classes of antihypertensives used world-wide.
In the population-based case-control study by Li et al, participants in the 3-county Seattle–Puget Sound metropolitan area were women aged 55 to 74 years, 880 of them with invasive ductal breast cancer, 1027 with invasive lobular breast cancer, and 856 with no cancer serving as controls. The exposures studied were recency and use of antihypertensive medications while the main outcome measures were risks of invasive ductal and invasive lobular breast cancers.
JUN
21
 In the June 2010 online version of the Lancet Oncology journal, a provocative report of a recently completed meta-analysis suggests that angiotensin receptor blockers might confer a modest but statistically significant increased risk for cancer.
In the June 2010 online version of the Lancet Oncology journal, a provocative report of a recently completed meta-analysis suggests that angiotensin receptor blockers might confer a modest but statistically significant increased risk for cancer.
These results were a mixture of both prespecified and non prespecified cancer outcomes in clinical trials where different ARBs were used though telmisartan was the study drug in approximately 86% of patients. Patients randomly assigned to receive ARBs had a significantly increased risk of new cancer occurrence compared with patients in control groups (7·2% vs 6·0%, risk ratio RR 1·08, 95% CI 1·01—1·15; p=0·016). When analysis was limited to trials where cancer was a prespecified endpoint, the RR was 1·11 (95% CI 1·04—1·18, p=0·001).
This meta-analysis does suggest a modest but significant link between cancer use and ARBs. However, questions remain. Firstly, is this affect real? Secondly, can we generalize these results to other medications within the ARB class. An important limitation of this study is that much of the data were derived from the occurrence of cancer in patients from the ONTARGET Study in the treatment arm where both ramipril and telmisartan were used; there was no effect seen in the monotherapy arms.*
At this point, more study is required. It is tempting to draw conclusions from this meta-analysis, however, we must remember that research in this area is actually conflicting. For example, it has been suggested that ARBs can actually be protective against cancer, as seen here.
Therefore, further study is warranted before concluding that this very useful class of medications is harmful and whether this is a drug or class-specific effect.
*Below is a copy of the Forest plot for the meta-analysis. As you can see, the effect of telmisartan on cancer from ONTARGET (the largest study), was only present in the combination group, not when used alone:
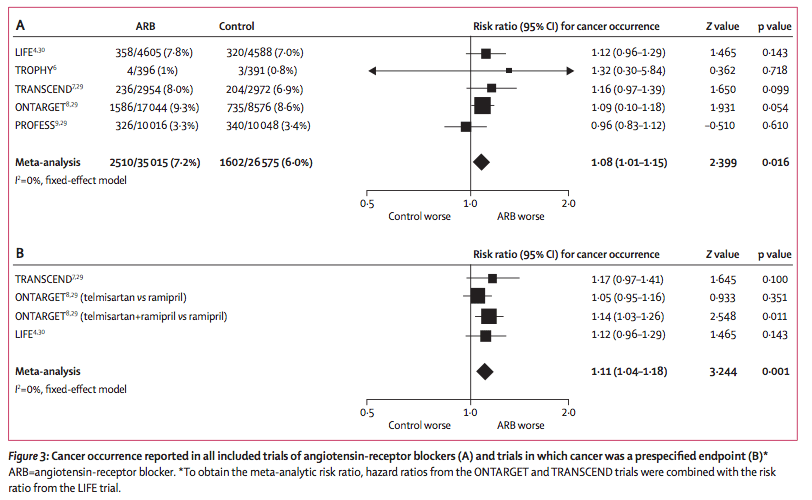
Source: The Lancet Oncology, Early Online Publication, 14 June 2010 doi:10.1016/S1470-2045(10)70106-6
MAR
12
The long awaited ROADMAP trial was recently published in the New England Journal of Medicine. This randomized controlled trial enrolled 4,447 patients to determine whether treatment with the angiotensin receptor blocker olmesartan could delay or prevent microalbuminuria.
In the study, blood pressure was targeted at less than 130/80 mmHg, yet patients randomized to the ARB group had a lower clinic blood-pressure by 3.1/1.9 overall. The time to onset of microalbuminuria was increased by 23% in the olmesartan group [hazard ratio for the onset of microalbuminuria 0.77; 95% confidence interval, 0.632 0.94; P=0.01]. However surprisingly, there was fewer cardiovascular deaths in the placebo group [3 versus 15, P=0.01].
DEC
20
 In a stunning development, Novartis said Tuesday that it will terminate the late-stage ALTITUDE study investigating Rasilez (aliskiren) in patients with type 2 diabetes and renal impairment on the recommendation of an independent data monitoring committee. The company indicated that the committee concluded that "patients were unlikely to benefit" from the addition of Rasilez to standard anti-hypertensives and also identified higher adverse events in this group (source: FirstWord).
In a stunning development, Novartis said Tuesday that it will terminate the late-stage ALTITUDE study investigating Rasilez (aliskiren) in patients with type 2 diabetes and renal impairment on the recommendation of an independent data monitoring committee. The company indicated that the committee concluded that "patients were unlikely to benefit" from the addition of Rasilez to standard anti-hypertensives and also identified higher adverse events in this group (source: FirstWord).
On a personal and professional note, these results come as a great disappointment to me. Not only does it suggest no further protection for our patients prescribed this strategy in an effort to reduce the burden of cardiorenal disease, but I was a great believer in the hypothesis and taught about it extensively throughout my career.
SEP
13
 It is prevailing wisdom that patients with chronic kidney disease (CKD) progress more slowly if their blood pressure is well controlled. In fact, most modern guidelines suggest that for patients with CKD, a blood pressure of 130/80 should not be exceeded.
It is prevailing wisdom that patients with chronic kidney disease (CKD) progress more slowly if their blood pressure is well controlled. In fact, most modern guidelines suggest that for patients with CKD, a blood pressure of 130/80 should not be exceeded.
In the latest issue of the New England Journal of Medicine, investigators cast doubt on this widely-held belief. In this anticipated report, patients with CKD but without proteinuria (<300 mg per day) and blood pressure targets of 140/90 fared equally well to those with blood pressure targets of 130/80. However, in those with protein excretion above 300 mg per day, the lower blood pressure target was superior. The authors conclude that in non-proteinuric patients, we should be targeting a less stringent goal of <140/90.
While these data are very interesting, one should pay close attention to what was considered proteinuria. A cutoff of 300 mg per day is a very low threshold; meaning, that many patients with hypertension may still benefit from the lower target. This trial is a very welcome one but take care not to paint all hypertensive patients with the same brush.
MAY
06
 Many studies have questioned the effectiveness of hydrochlorothiazide (HCTZ) versus chlorthalidone as a diuretic. In fact, most large scale trials that have used HCTZ have been disappointing (e.g. ACCOMPLISH) while those using chlorthalidone have been largely positive (e.g. ALLHAT). While this might seem like an over-simplification, many hypertension experts agree with it.
Many studies have questioned the effectiveness of hydrochlorothiazide (HCTZ) versus chlorthalidone as a diuretic. In fact, most large scale trials that have used HCTZ have been disappointing (e.g. ACCOMPLISH) while those using chlorthalidone have been largely positive (e.g. ALLHAT). While this might seem like an over-simplification, many hypertension experts agree with it.
In the latest twist to this story, Takeda Pharmaceuticals have created a fixed dose combination with it's new ARB azilsartan with chlorthalidone - in stark contrast to all other ARB and ACE inhibitor counterparts. As it it turns out, they may be on to something ( continued ... )
MAR
15
 Much has been written over the years of a so-called J-point in blood pressure management; that point above which BP is too high and below which BP is too low (if one is arriving there by antihypertensive medications). The late breaking ACCORD BP Study, published online in the New England Journal of Medicine, casts doubt on the benefit of aggressively lowering systolic blood pressure towards 120 mmHg in patients with type 2 diabetes.
Much has been written over the years of a so-called J-point in blood pressure management; that point above which BP is too high and below which BP is too low (if one is arriving there by antihypertensive medications). The late breaking ACCORD BP Study, published online in the New England Journal of Medicine, casts doubt on the benefit of aggressively lowering systolic blood pressure towards 120 mmHg in patients with type 2 diabetes.
However, while much will be written on these very results, I want to issue a cautionary note that this trial not be interpreted as 'strict blood pressure management is unimportant'. Quite the contrary; tight blood pressure control is likely more important that tight glycemic control in patients with type 2 diabetes, but there is a limit to this effect. The ACCORD BP study should be interpreted as nothing more than the demonstration of a J-point in blood pressure management, a finding that actually support current published guidelines in patients with diabetes to target a BP below 130 rather than an even stricter threshold (NB: 130 as a target has not been firmly established by randomized trial data). We now understand however, that 'below' is not a bottomless term and that a range of 120 to 130 is likely appropriate.